Various predecessors of modern sutures developed very early. The first indications of surgical suture methods were discovered by researchers in 5,000-year-old Egyptian scriptures, which show, among others things, the illustration of a suture needle with an eye. In addition to plant fibers, another common suture material of the early period were tendons. Later, textiles such as linen were used more and more often. Clear traces of textile suture material were detected and verified on a mummy dated 1000 B.C.

However, wound infections were often the result of using unclean, germ-laden instruments and materials. This did not change until the English surgeon Joseph Baron Lister and his German colleague Curt Theodor Schimmelbusch independently implemented the first usable disinfection and sterilization procedures at the end of the 19th century. From 1868 Lister used gut strings as suture material and disinfected them with carbolic acid – this marks the origin of the first catgut. Advantage of the material obtained from sheep or bovine intestine: It dissolved gradually into the wound without leaving a residue and could be absorbed by the body. With the BSE crisis in the early 2000s, the use of catgut declined rapidly in favor of synthetic materials.
Modern suture materials
While sterility is a basic requirement nowadays, modern suture materials have to meet completely different and multifaceted requirements. In addition to excellent gliding properties of the thread when passing through the tissue to be operated on, high tear resistance and knot security are among the crucial criteria.

Modern surgical suture material is made of synthetic or natural materials in numerous variations.

Needle and thread are swaged, meaning firmly connected. This ensures that there is as little tissue damage as possible during surgery.
As extensive as the requirements for the thread are, the thread itself is just as varied. Synthetic or natural materials are twisted or braided into monofilament (single-fiber) or multifilament (multi-fiber) thread variations. Other options include sheathing or coating of resorbable or non-resorbable threads.
The designs and shapes of modern suture needles are also extremely complex and versatile. To make sure that tissue damage during surgery is kept to a minimum, needle and thread are swaged. This means firmly connected, to keep the needle as thin as possible, rather than pulling a large needle eye through the tissue. Every needle-thread-combination has its own special features which the surgeon, depending on wound and surgical technique, has to take into account when making his choice.
Sophisticated production process
There are some challenges to overcome in manufacturing surgical suture material. After the needle-thread-connection has been swaged, the needle is fastened in the so-called needle park of the thread carrier, the tray. The thread is then wound on the tray with up to 800 revolutions per minute and ultrasonically welded with a paper lid. On the one hand the lid serves as a batch information area and lists the specifications of the needle-thread-combination. On the other hand, it serves as a drying agent in order to ensure a constant quality of the suture material.

The swaged needle-thread-connection is fastened in a tray.
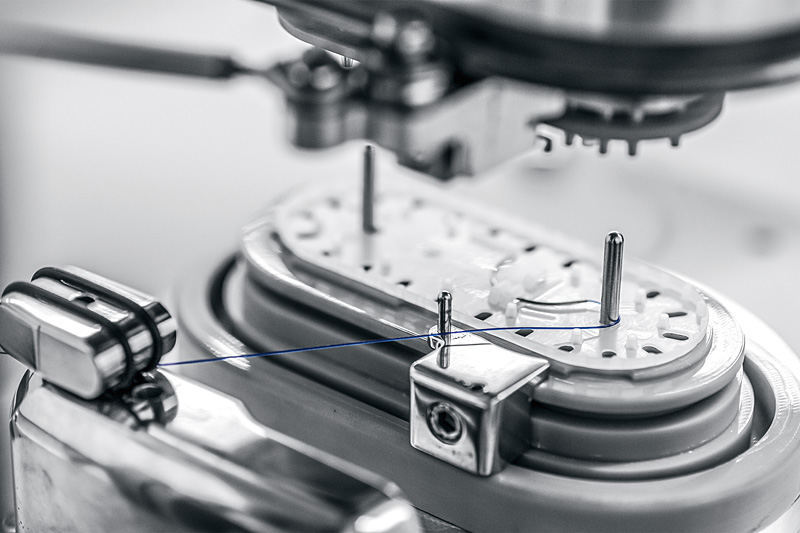
Then the thread is wound on the tray with up to 800 revolutions per minute.
During the winding process it is particularly important to control the thread and to make sure that it does not end outside the tray. Various cameras help to comply with the high quality requirements.
Sterile packaging
When packaging surgical suture material, the trays are placed in the molded cavity of an aluminum blister. The lid foil applied to it has a tear-resistant, puncture-proof and breathable Tyvek window which enables sterilization by ethylene oxide gassing. During drying of the gassed blister, the moisture escapes through the Tyvek window, which is subsequently removed. Finally, the blister containing the suture material is sealed completely tight.
Download this article as PDF file
Photos: Helmar Lünig